class ii malocclusion treatment adults
Even so a recent study has. Applying sound biomechanical principles to execute the mechanics plan is the surest way to achieve predictable results with minimal side effects.

Treatment Of Class Ii Division 2 Malocclusion In Adults Biomechanical Considerations Jco Online Journal Of Clinical Orthodontics
2 In the present case orthodontic treatment was a reasonable alternative for an adult patient without significant skeletal discrepancies.

. In both groups the soft tissue profile convexity was reduced significantly. 1 Description of changes in the position of the upper and lower lips as a result of the change in the position of upper and lower incisors after orthodontic treatment of malocclusion of Class II division 2 type. When planning the treatment in such cases the orthodontist often faces the di-lemma whether to extract 2 maxillary premolars or 2 maxillary and 2 mandibular premolars.
For the treatment of Class II div 1 malocclusion various treatment modalities have been presented. Ideally treatment of Class II malocclusions should focus first on improving the skeletal discrepancy using functional appliances while the individual is still growing. Significant reductions in profile convexity are achievable.
3 For growth modification three types of orthodontic appliances are used. By using the biomechanical concepts with specific objectives in mind the clinician can achieve the desired goals. Early treatment costs more money in.
Time with increased efficiency and reduced cost1 Class II malocclusion can be treated by several means according to the characteristics associated with the problem such as antero-posterior discrepancy age patient compliance2 In adolescents the correction of Class II malocclusion by growth modification is the treatment of choice3-5. The best treatment modalities for class II malocclusion in growing patients include using functional appliances either removable Activator Bionator Frankel and Twinblock or fixed appliances MARA cemented Twinblock or Herbst appliance that mostly enhance further mandibular growth via mandibular advancement and also headgear Cervical Highpull and. The CMA appliance is an efficient and effective way of correcting Class II malocclusion.
Following careful diagnosis and treatment planning the first step of treatment is usually to start improving the deep bite by intrusion and. However in an adult the latter two are the only options. In a growing patient all three may be possible.
This overbite can be caused by an overly prominent upper jaw or an underdeveloped lower jaw. 2 Determination of correlation between changes in the position of lips and incisors in the profile of the face after orthodontic. 1 However dentoalveolar compensations reducing overjet and the severity of the Class II malocclusion are still the major effect of functional appliances.
Pre-treatment proclined mandibular incisors limit the scope of indications for fixed functional appliances as they can cause an increase in lower incisor proclination. An electronic search was performed in MEDLINEPubMed Embase Scopus. 1 Types of studies.
Abstract and Figures. Class III malocclusion camouflage treatment with. The treatment of an adult Class II patient requires a careful diagnosis and a treatment plan which involves aesthetic occlusal and functional considerations.
The aims of our research were as follows. To perform the correction of class II malocclusions in adult patients extractions may include two maxillary premolars and two mandibular premolars. Treatment of Class II division 1 malocclusion includes growth modification orthodontic treatment and orthognathic surgery.
23 In adults repositioning of the maxilla and. 2 Extractions of only the upper premolars are indicated when there is no crowding or cephalometric discrepancy in the mandibular arch3 4 These are probably the most extracted teeth for orthodontic purposes. For a skeletal Class II malocclusion three treatment alternatives exist ie Growth modification Dental camouflage Orthognathic surgery.
This case report presents. Herbst appliance therapy can be considered a modality for the. The changes were mainly dentoalveolar in.
Randomized or non-randomized clinical studies prospective or retrospective. The mode of correction of the Class II malocclusion was through skeletal and dental changes. Nongrowing individuals with Class III malocclusion undergoing orthodontic camouflage treatment.
Simultaneously stimulating mandibular growth. On the other hand in adult patients with severe Class II malocclusions generally involving extremely deficient mandibles orthognathic surgery is often the only possible treatment. Class II division 1 malocclusion is described as the incisal edges of the lower incisors occlude posterior to the cingulum plateau of the upper incisors and the upper central incisors are proclined 1.
Definition of a class 2 malocclusion. The indications for the extractions in the orthodontic practice have historically been controversial 1113. Class 2 or class II malocclusions are characterized by upper molars that are too far forward compared to the lower molars.
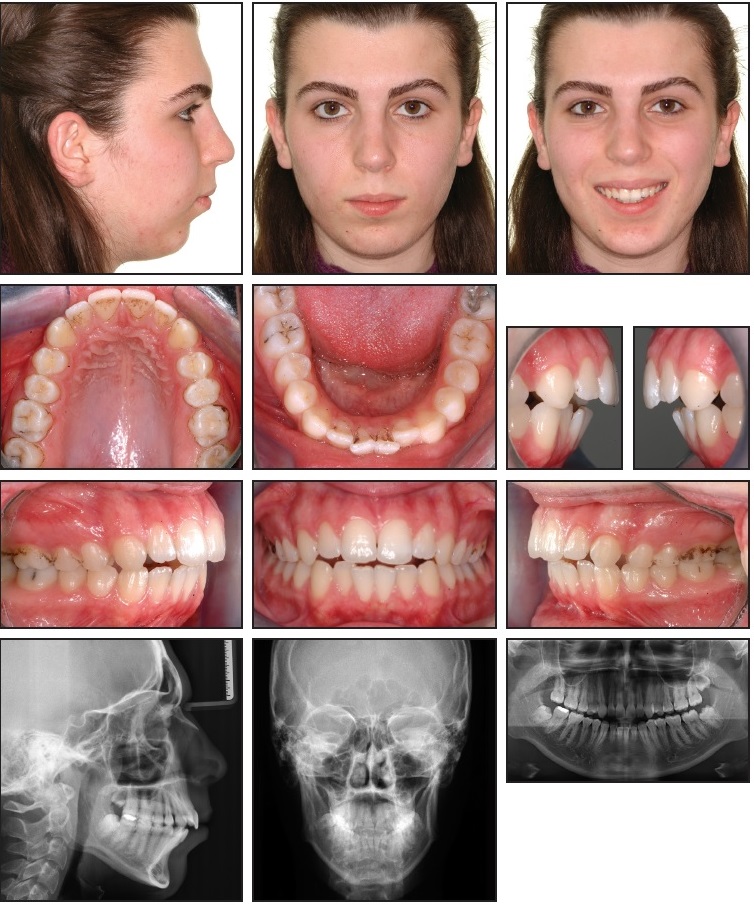
Asymmetric Class II malocclusion left subdivision mandibular midline shifted to the left mild mandibular anterior crowding excessive overbite 4-mm overjet and a brachycephalic facial pattern. These cases are often characterized by severe traumatic deep overbites with lingually inclined upper incisors. Young adults who desire cost effective non surgical correction of Class II malocclu-sion and accept dental camouflage as a treatment option to mask the skeletal discrep-ancy.
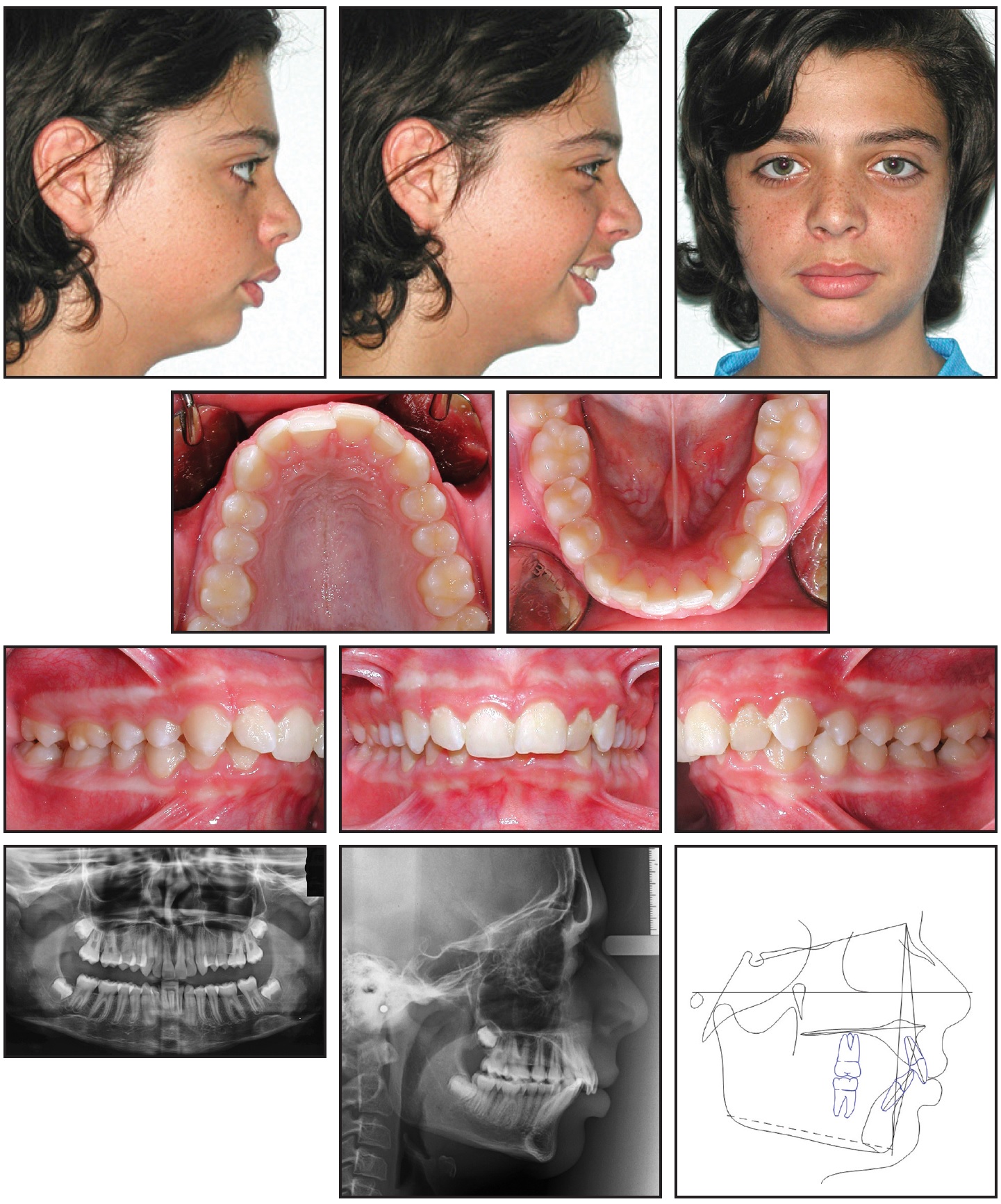
This case study features a 15 -year old female with a Class II division 1 malocclusion an orthognathic maxilla and an 8mm overjet. The prevalence of this malocclusion varies amongst different populations but it is reported to be 20 in the UK 2. Early treatment phase 1 as part of a two-phase treatment to correct Class II malocclusion is rarely indicated as it is not effective and incurs greater cost than one course of treatment with fixed appliances provided when the child is in adolescence.
To evaluate the effects of camouflage treatment of Class III malocclusion in adults. Dental malocclusions are classified based on the positioning of the upper and lower molars. Treatment of Class II division 2 malocclusion in adults is always challenging.
No one ever had any problems because their molars are half a unit 2-3 mm Class II. Treatment of an adult Class II patient requires careful diagnosis and a treatment plan involving esthetic occlusal and functional considerations5-7 The. Treatment of a Class II division 2 malocclusion is a challenging issue for orthodontists.
Because of their limited skeletal effects and minor changes in the profile they are indicated only in patients with a moderately severe Class II malocclusion. Treatment goals included achieving functionally optimal and aesthetically acceptable occlusion eliminating dental arch crowding reducing. Although camouflage may be attempted by extracting premolars the soft-tissue objectives may be impossible to meet.
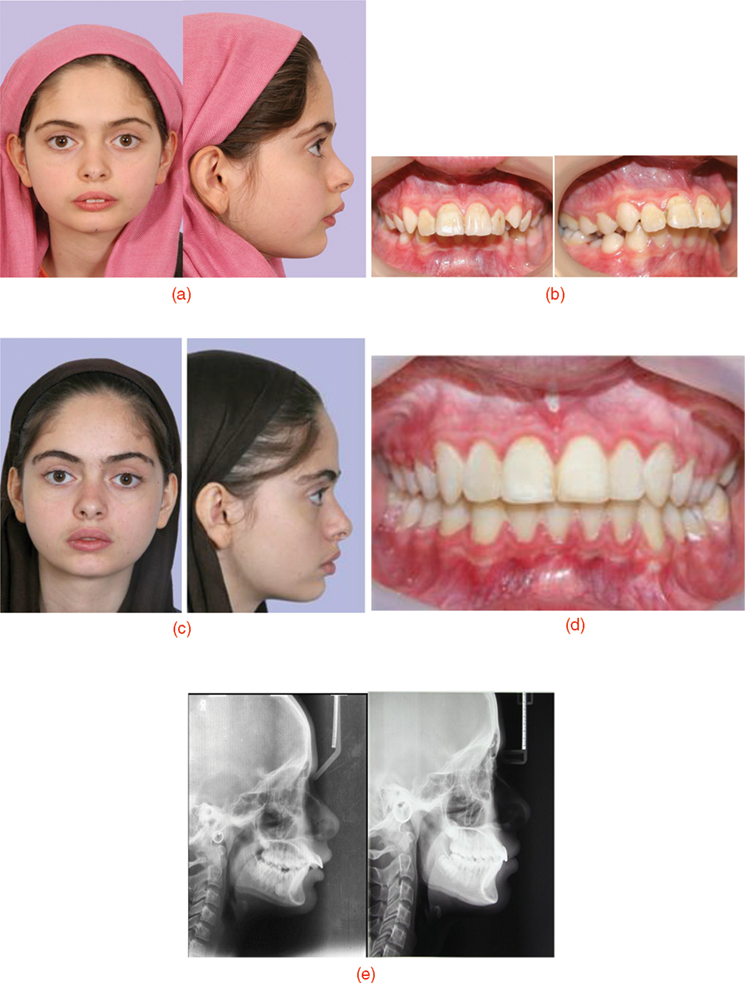
This paper aimed to describe the orthodontic treatment of an adult patient with the following characteristics. The premolars are probably the most commonly extracted teeth for orthodontic purposes as they. However in the stepwise sample the amount of correction due to skeletal changes was higher.
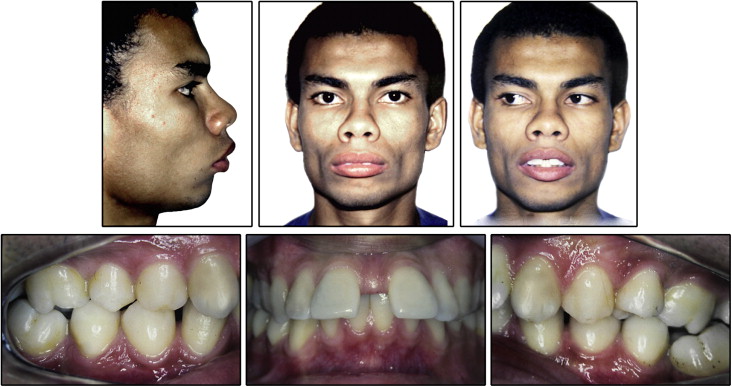
To be included in the review studies had to meet the following inclusion criteria. They are - Extra oral force appliance Functional appliance. A 31-year-old male patient treated with fixed preadjusted.

Figure 1 From Treatment Of A Young Adult Patient With Class Ii Division 2 Malocclusion By Using Forsus Fatigue Resistant Device 2 Years Follow Up Semantic Scholar

Pdf Orthodontic Camouflage Treatment Of Class Ii Malocclusion In Non Growing Patient A Case Report Semantic Scholar

Treatment Of A Severe Class Ii Division 1 Malocclusion Combined With Surgical Miniscrew Anchorage American Journal Of Orthodontics And Dentofacial Orthopedics
Case Report Jco Online Journal Of Clinical Orthodontics

Treatment Of Class Ii Division 2 Malocclusion In Adults Biomechanical Considerations Jco Online Journal Of Clinical Orthodontics
Functional Class Ii Treatment With A Miniplate Anchored Herbst Appliance Jco Online Journal Of Clinical Orthodontics

Class Ii Treatment Photos Orthodontics Cary Nc Clayton Nc

Class Ii Treatment Photos Orthodontics Cary Nc Clayton Nc

Management Of Skeletal Class Ii Malocclusion By Surgery First Approach A Short Term Clinical Experience Semantic Scholar
Is Traditional Treatment A Good Option For An Adult With A Class Ii Deepbite Malocclusion Pocket Dentistry
Advances In Management Of Class Ii Malocclusions Intechopen

Pdf Treatment Of Class Ii Division 2 Malocclusion With Miniscrew Supported En Masse Retraction Is Deepbite Really An Obstacle For Extraction Treatment Semantic Scholar
Advances In Management Of Class Ii Malocclusions Intechopen
2
Treatment Of A Class Ii Division 1 Malocclusion With The Combination Of A Myofunctional Trainer And Fixed Appliances American Journal Of Orthodontics And Dentofacial Orthopedics

Treatment Of Class Ii Malocclusion With Tooth Movement Through The Maxillary Sinus American Journal Of Orthodontics And Dentofacial Orthopedics

Nonsurgical Treatment Of Severe Class Ii Malocclusion With Anterior Open Bite Using Mini Implants And Maxillary Lateral Incisor And Mandibular First Molar Extractions American Journal Of Orthodontics And Dentofacial Orthopedics

Class Ii Treatment Photos Orthodontics Cary Nc Clayton Nc

Treatment Of Class Ii Malocclusion With A Customized Lingual Appliance Combined With A Class Ii Corrector American Journal Of Orthodontics And Dentofacial Orthopedics